If you or someone you know may be experiencing a mental health crisis, contact the 988 Suicide & Crisis Lifeline by dialing or texting “988."
Someone in America dies by suicide every 11 minutes. It’s that common. But not normal.
Humans have evolved over centuries to survive. So when people try to kill themselves, something has gone wrong. Typically, the assumption is that something happened in the person’s mind — a mental illness.
But in recent decades, there’s been a growing movement to ask a different question: What went wrong in the world around that person?
For Chris Pawelski, it was a torrent of factors. His dad — one of his best friends, whom he worked with daily for decades — was diagnosed with renal cancer and died six months later. Pawelski was left as the primary caregiver for his mom, who had dementia.
His family’s in New York’s Orange County — where he first worked as a 5-year-old, collecting onions that fell out of crates — was hemorrhaging money. Pawelski said he was growing roughly $200,000 worth of crops some years but took home only about $20,000, unable to negotiate higher prices with wholesale buyers that dominated the market.
Debt to suppliers and equipment vendors piled up, and the burden strained his marriage. He had little time for friends, working sunup to sundown seven days a week, desperately trying to preserve his family’s legacy.
“It’s all stuff collapsing down upon you,” he said. “It’s weeks, months, years of dealing with all sorts of pressures that you can’t alleviate.”
Pawelski started wondering what it would be like to get hit by a truck on the busy road in front of his house. “You think you’re already on your way out, so why wait?” he said.

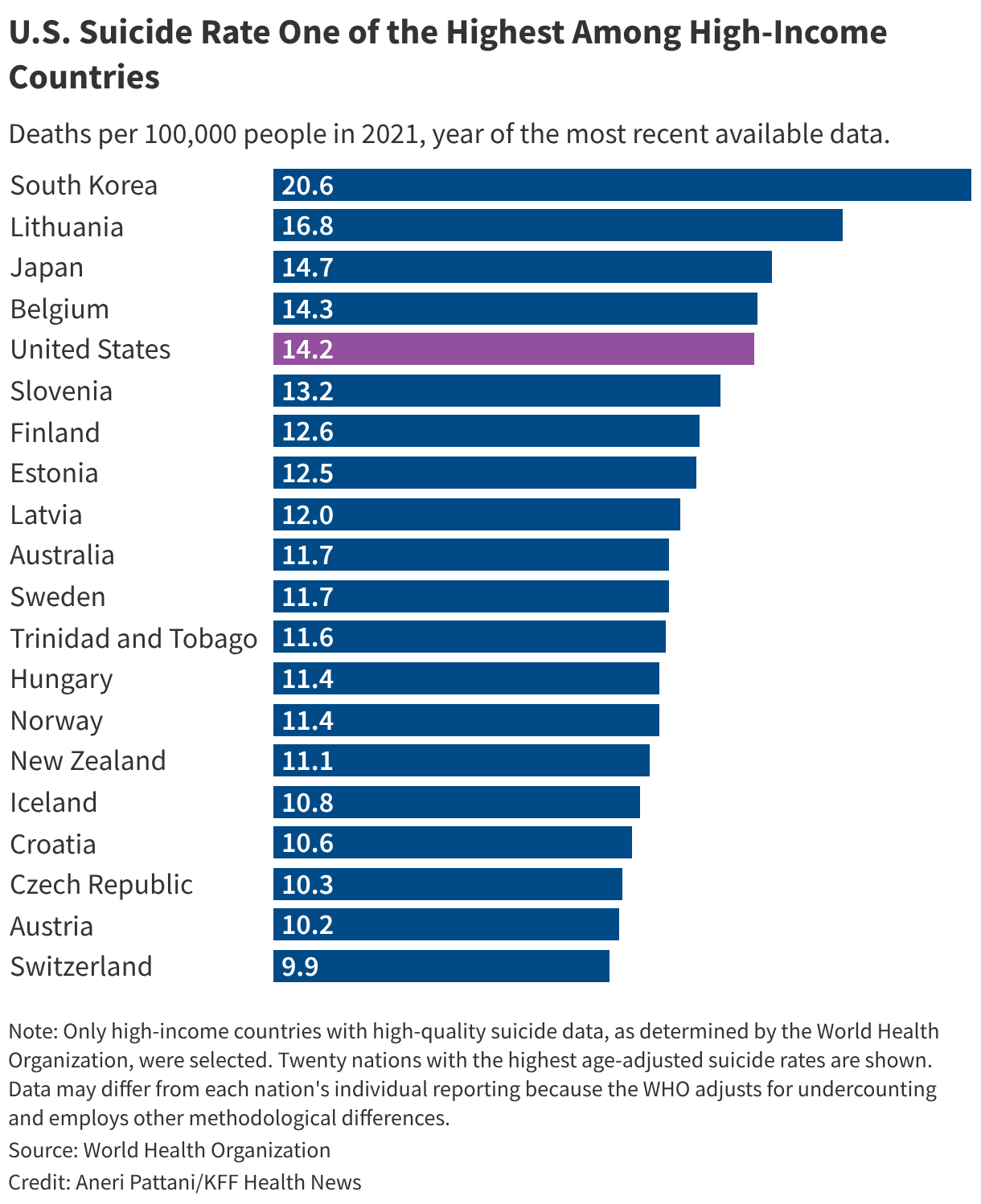
Millions of Americans have , and tens of thousands . Suicide repeatedly ranks among the — making the U.S. an .
Prevention efforts have typically focused on connecting individuals in crisis with treatment — despite therapy and medication being , the healthcare system , and a consensus that suicide is caused by a , including but not limited to mental illness.
Now, many people working to prevent suicide, including some who have tried to harm themselves or lost a loved one to it, are calling for a broader approach. Some were galvanized by the covid pandemic, when rates of — not because everyone’s brain chemistry suddenly changed but because the world changed. That led many to believe that, while treatments and crisis care are vital, the goal of suicide prevention needs to expand beyond stopping people from dying to also giving them reasons to live.
“It’s not rocket science,” said , a psychologist and internationally recognized suicide prevention researcher who lost her brother to suicide. If “you have happier, healthier people, they live longer, happier lives.”
That means suicide prevention shouldn’t be limited to answering hotlines or treating patients in psychiatric wards, she said. It should also involve running food banks to ensure families don’t go hungry or hosting weekly book clubs for homebound seniors to make friends. It can take the form of school programs that build resilience in children or housing policies that prevent evictions.
shows these — even if they don’t have the words “mental health” or “suicide” in the title — can reduce the number of people who kill themselves. They often lower rates of crime, addiction, and poverty, too.
The U.S. has lagged other countries in adopting this approach, Spencer-Thomas said, perhaps because it’s easier — and more politically palatable — to tell someone to go to therapy than it is to enact sweeping policy changes, such as an .
“As long as we have that convenient narrative that it’s just a bunch of broken people needing medicine and treatment, then we’re never accountable for fixing the broken things in our communities,” Spencer-Thomas said.
The Trump Administration’s Approach
Overhauling suicide prevention efforts to focus on broad social and economic policies might seem overwhelming and unrealistic — especially right now. This approach requires large upfront investments that lack across-the-board support, either because of budgeting realities or ideological bents.
President Donald Trump and his appointees have said little about suicide directly, but many of their policies do the opposite of what shows .
The administration has championed and the that are projected to leave and in coming years. It has injected uncertainty into the economy through , , and . It has for school-based mental health initiatives, gutted federal programs that focus on at-risk blue collar workers, and . (Suicides are the in America.)
“All of these changes are creating a firestorm,” said , the chief advocacy officer for the National Alliance on Mental Illness. They can cause “extreme stress and anxiety” in people’s lives, she added, and “when people feel desperate, that’s when crises can emerge.”
Federal health officials insist that suicide prevention remains a priority.
, director of the Centers for Disease Control and Prevention’s injury center, said the agency is focused on creating systems that can support people “no matter what may be happening” in the world around them. “There’s always going to be turmoil in people’s lives,” she added.
Arwady and , who leads suicide prevention work at the Substance Abuse and Mental Health Services Administration, said several of the Trump administration’s priorities align with an upstream approach.
For example, they said, its could help address the , since exercise is proven . Similarly, people who are homeless have , and the administration has been . Federal officials have also encouraged , and research shows members of faith communities are .
However, the Trump administration has made at and and has for , leading to questions about whether or how this work will continue.
A History of Medical and Crisis Care
Suicide prevention reached the national stage in the late 1990s, said , who worked at the CDC for 15 years before joining the , a nonprofit focused on teen and young-adult mental health.
As suicide rates grew among young people, a group of government officials, clinicians, and advocates gathered in Reno, Nevada, in 1998 to discuss the pressing issue. Over the next few years, the surgeon general and the federal government published its .
These documents acknowledged the role of society and economics in suicide risk but focused heavily on identifying people in crisis and increasing access to medical treatment.
Those are critical steps to suicide prevention, many mental health researchers and clinicians say. They’re also politically favorable. For elected officials, who have a few years to demonstrate their achievements before the next campaign, it’s easier to count the number of people receiving therapy than the number of people who never developed suicidal thoughts because long-term economic and social investments helped them maintain steady jobs and strong friendships.
The push for individual treatment also comes from a pervasive misconception that suicide is always the result of an underlying mental illness, said , who is the senior director of population health at Mental Health America and contributed to a .
Although how many people who die by suicide — with estimates from to — the takeaway is that mental illness is not the sole cause, Reinert said. That means treating it can’t be the sole response.
Plus, mental illnesses can be by life circumstances. Treating depressive symptoms without looking at factors such as childhood trauma, the loss of a loved one, or being laid off from a job is an incomplete approach, many mental health researchers and clinicians say.
The covid pandemic, especially, made people in the field recognize “we really need to address all of these conditions that are creating stress, anxiety, and crises,” Stone said.
In July 2022, the federal government — a shorter number for the national suicide crisis line, meant to provide an alternative to 911 for mental health emergencies.
, who led federal work on 988, said the infusion of money and attention on the hotline helped states build better crisis response systems, from centers that answer calls to mobile crisis units.
But that’s not enough to solve America’s suicide problem, she said. “You’ll never be able to build a system based on crisis alone.”
Help for the Farm and the Farmer
Pawelski, the onion farmer in New York, hit his breaking point in 2020.
He had a decent crop that year, but Canadian exporters were into American markets, making it difficult for him to sell his product.
“I was having to beg people” to buy, he said. And when he managed to sell, prices were comparable to prices in the 1980s.
By the end of the season, he had incurred losses of a few hundred thousand dollars.
He said he and his wife decided, “We couldn’t afford to grow onions again.”
The idea that his family’s onion farm would end with him was “soul-crushing,” Pawelski said. He lost weight rapidly and thought about ending his life.
He and his wife called for help. Founded at Cornell University in 1986, the free program connects farmers with two consultants: a financial analyst specializing in farm planning and a social worker focused on emotional concerns and family dynamics.
The financial specialist helped Pawelski develop a new business plan. Instead of farming onions for wholesale, he could grow greens, tomatoes, peppers, and eggplants at a small scale to sell directly to consumers. He could upgrade an old truck with a cooler and deliver produce to people’s doors. He would supplement that income with teaching, speaking engagements, and other work that took advantage of his master's degree in communications.
The social worker helped him accept that new reality — equally crucial, Pawelski said. “If you’re pissed off” about the change, “no matter what kind of proposal or idea they have, it’s not going to go anywhere.”
The adjustment took months. Pawelski also saw a therapist during that time.
Then one day a neighbor noted that Pawelski seemed much happier. That “caught me off guard,” Pawelski recalled. He didn’t realize his inner transformation was so apparent.
Today, Pawelski’s business has stabilized, and he and his wife are paying down debt. Pawelski advocates for programs to help farmers’ mental health and address their .
That can mean crisis hotlines and access to affordable therapy, Pawelski said. But what he really wants are policy changes that help farmers get fair prices for their produce, debt relief, and the installation of broadband internet in rural areas so farm families and employees can be connected.
“We need to think broader and longer-term than a helpline,” he said. That’s “a band-aid on a gunshot wound.”

Ńîąóĺú´«Ă˝Ň•îl Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about .